Since my diagnosis of metastatic prostate cancer (meaning it had spread) in August of 2018, I ve been working hard trying to figure out what went wrong, and what I could have done differently. What I discovered was that there was a lot I didn t know about prostate cancer - things I wish my doctor had told me but didn t. (They were things that my doctor probably didn t know either.) I was getting regular check-ups and getting my PSA checked, and DREs (good ol' digital rectal Exams) but my PSA was below the "safe threshold" I was given, so the fact that my doctor thought she felt a bump with her finger didn t set off warning bells like it should have. I learned the hard way. There were also issues with the standard of care that was being used, in particular with the universal safe PSA threshold of 4.0 that my doctor adhered to. I hope that no one else has to go through what I m going through, so I did a lot of research and I created a fairly comprehensive brochure on the basics of prostate cancer and on the potential value of DREs and PSA screening. (The pamphlet is below and PDF copies are attached.)
Not only did I spend a great deal of time on this, I ve also reviewed it with a number of people with their own experience with prostate cancer who provide me with valuable input and editing commentary. If you are a male over 50, please take the time to read through this and hopefully you will learn some things. If you have any questions, feel free to contact me. My e-mail ID is: runlikehal@yahoo.com. I will make every effort to reply to any serious questions. Be well... -Hal

Citation References used in Run Like Hal's info flyer:
1) Possible Warning Signs for Prostate Cancer: Here is a link to the Prostate Cancer Foundation and their list of 10 warning signs of prostate cancer. But note that this is the statement that they open with: "Unfortunately, there usually aren t any early warning signs for prostate cancer. The growing tumor does not push against anything to cause pain, so for many years the disease may be silent. That s why screening for prostate cancer is such an important topic for all men and their families."
Link to PCF site with prostate cancer warning signs
2) Prostate Cancer Mortaility: Here is a link to the National Cancer Institute (part of the NIH) with the stats I quoted regarding prostate cancer deaths. Note, there is an apparent incongruity between the graph which indicates ~ 19,000 deaths per year where as they state above the graph that 30,000 deaths are expected in 2018.
Link to NCI site with stats on prostate cancer mortality rate
3) DRE Exam Info: Here are a number of links that give an idea of what you can find from a DRE (Digital Rectal Exam) of your prostate. They all pretty much say the same thing.
Link to Healthline.com site with DRE info
Link to Prostate Caner of Canada with info on how the prostate should feel
Link to Stanford Medicine website with info on how to perform a DRE and what find
4) PSA "Safety Threshold": There are a number of different standards for the "safe PSA threshold". I very much favor one that is age differentiated. For reasons unclear, the National Cancer Association gives a blanket 4.0 standard. They need to update that, as it allows people like me to slip through. The age graded standard taht I have included in my pamphlet is this one.
Link to MedicineNet.com PSA chart (You need to scroll about halfway down the page.)
PCF chart for PSA levels that is similar to MedicineNet, but differs for my age range (they list 4.0 for 50 - 59, vs 3.5) and due to that I don't support it.
Link to American Cancer Society website. that indicates the universal 4.0 value that my doctor used, which may eventually cost me my life. (That maybe a bit dramatic, but true.) The ACS does indicate that some people use lower values, and that age and race may be a factor. I feel strongly that they need to formally adopt an age and race adjusted scale.
5) PSA Velocity: There are likely many other sites with info on PSA velocity, or rate of change per year, but this is one that I have found with useful info.
Link to a website with PSA velocity info that I quoted in my flyer.
6) PCA 3 test: PCA3 (prostate cancer antigen 3 gene) test involves getting a prostate massage then producing a urine sample. It is a relatively new test, but it does correlate better for the presence of cancer than a standard PSA test. Below are two links from HealthLine.com.
However, as they state: The prostate cancer antigen 3 gene (PCA3) test is used to help determine your risk of prostate cancer. It is not used to diagnose prostate cancer.
It s mainly used to determine if your elevated prostate-specific antigen (PSA) levels are likely caused by prostate cancer. PSA is a protein produced by cells in your prostate. Elevated levels of this protein could indicate a harmless problem with your prostate, such as an enlarged prostate. But elevated PSA levels can also indicate prostate cancer.
Healthline.com link on PCA3 test info
7) MRI vs Biopsy: Ok, I admit, this issue both confuses me and make me angry. Common sense should make it clear that any man given the choice would prefer to have a non-invasive MRI vs a biopsy if they can gather similar relevant information. Guess what - they can! Certainly a biopsy will be needed at some point if cancer is detected / suspected, but an MRI first can help confirm if cancer is present, and if it is detected on the MRI, that info can be used to guide the biopsy samples taken. Doing an MRI first makes very basic common sense and medical sense for those reasons. For reasons unclear , the standard of care in the U.S. is to get a biopsy first, and an MRI second. However in the UK, they are making a "radial leap" and are now espousing doing the MRI first. So are the U.S.s medical standards really behind those of the UK with their Socialized Medicine? You bet yer sweet bippy they are. The U.S. needs to get on the stick. This one also may cost me my life, so God dammit, someone in the U.S. needs to get a grip on some common sense for this very simple issue, and I sure do mean that. Here are a number of links, all from the UK that discuss this incredibly logical strategy.
The Telegraph News Science link on MRI vs biopsy.
Penningtons link on MRI vs biopsy.
Another Penningtons link on MRI vs biopsy.
8) Risks due to a naturally high level of testosterone: this one may haunt me until the day I die. I'm fairly certain that I had a naturally high testosterone level, but I never had it tested. I didn t know that testosterone feed the growth of prostate cancer. When I found out about this and confronted my doctor, I was told "Studies have not shown any link to increased risk of prostate cancer to high testosterone levels." My immediate reply was, "Ok, but if someone does have cancer, a high testosterone level sure will make it more likely to grow and spread" I didn't have to do any research to figure that out - it was common sense. If testosterone is the fuel that feeds the growth of the cancer fire, more if it will help it spread faster. (If someone can prove me wrong on this, have at it.) After I was diagnosed with cancer, I asked my Urologist for a testosterone test, but he ignored my request. (I suppose he figured it was too late at that point, and if I was right, it might not look good for my primary doctor.) I also asked my primary for a test, but I had already started taking drug therapy, so I figured the test would no longer be accurate, so I let it go. Only later did I discover that the drug I was on initially (Casodex) would not have made the test inaccurate as it does not suppress testosterone production. My primary physician thought I had a nodule on my prostate for some time (years) but never suggested this test. I sure wish that test was performed.
I normally wouldn t quote a drug company, but here is a direct statement from a Ferring Pharmaceuticals website: Cancer of the prostate gland develops when cells of the prostate show uncontrolled growth. High levels of testosterone help fuel prostate cancer growth.
Here is the link to that info: Ferring site for their Firmagon anti-androgen drug.
9) 20% of prostate cancer is aggressive: I got this info from an NBC News story that quotes Dr. Edward Schaeffer, chair of urology at Northwestern University Feinberg School of Medicine and Northwestern Medicine, who led the study in question. As is stated in the interview: "3% (of prostate cancer) had metastasis on diagnosis, the remainder had localized disease: 32 percent low, 45 percent intermediate and 20 percent high risk." (This quote is about half way down the article.)
Note - on the bawdy quote I provide that playing Russian Roulette with a six-shooter is less risky than not getting prostate cancer screening, the basis of that is that 20% is 1 out of 5, and one bullet in a six-shooter is 1 out of 6, which is a slightly lower odd of something bad happening than 1 out of 5. I don't think most people would be willing to play Russian Roulette with a live round in a gun, and yet many men do avoid prostate screening tests. I think that is a bad idea, as I hope is made quite clear by my statements, flamboyant or otherwise.
Here is a link to the NBC story: NBC News story regarding aggressive prostate cancer.
If you want to open / download PDFs of the flyer, or get more info about how I put it together:
Prostate Cancer Info Pamphlet pages 1&2
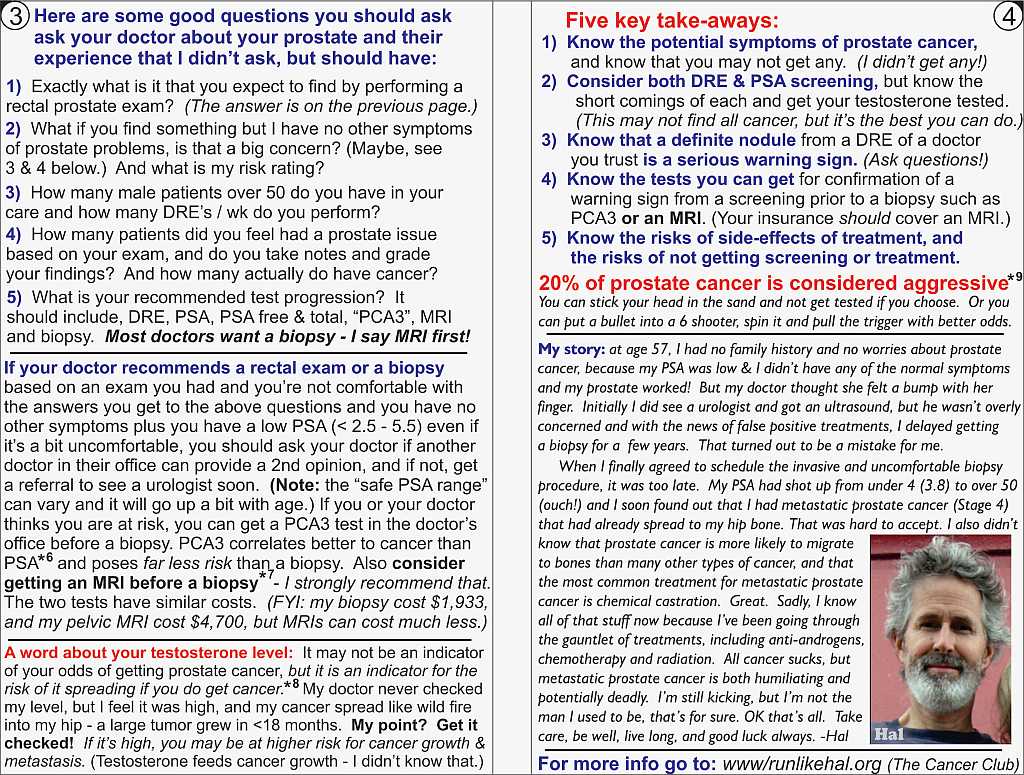
Prostate Cancer Info Pamphlet pages 3&4
Prostate Cancer >*< reference info
Commentary about the making of this flyer